

.svg)





Parent Guide to Speech Sound Milestones: Understanding Articulation & Phonology in Children
Speech sound milestones are more than a checklist of when children should say certain sounds. They are closely tied to later language, literacy, and academic outcomes, and they guide decisions about whether a child is developing at their own pace or needs targeted support. For parents and speech-language pathologists, understanding articulation development and phonology is essential to answering a simple but important question: “When should my child say sounds?”
This guide brings together current, research-based articles on speech sound milestones, explains articulation and phonology in easy to understand language, and translates the evidence into practical strategies for home use and therapy setting.
What Are Speech Sound Milestones?
Speech sound milestones are age ranges during which most children (typically 85% or more) can correctly produce particular consonant sounds in their language. The milestones are based on large normative studies and clinical guidelines and used by speech language pathologists to determine whether a child’s speech sound system is age-appropriate.
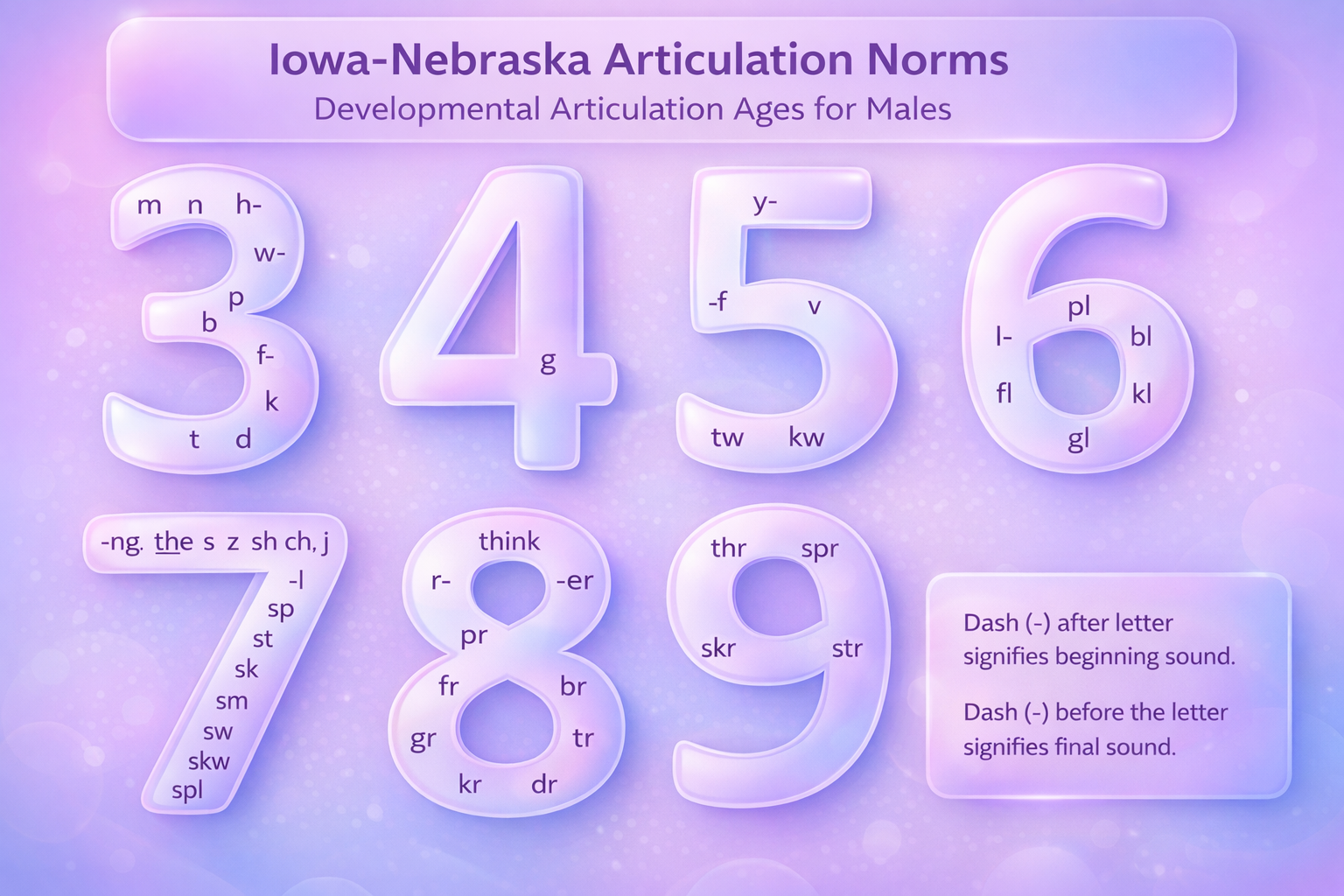
There are several well-established resources that help contextualize speech sound development. For a broad accessible overview of typical speech sound acquisition patterns across early childhood ASHA’s developmental speech and language milestone chart offers great guidance. For more specific milestones the Iowa–Nebraska articulation norms provide a detailed chart of age-of-acquisition benchmarks for English consonants and clusters through age five. In addition, based on Shriberg’s seminal work, the study on early-, middle-, and late-developing sounds by Fabiano-Smith & Goldstein (2010) provides a clinically useful framework for understanding relative sound complexity and expected mastery timelines in Spanish speaking children. Together, these resources support evidence-based decision-making and reinforce the importance of interpreting speech sound development within a structured, developmental framework rather than in isolation.
Why Speech Sound Milestones Matter for Long-Term Outcomes
Speech sound development does not occur in isolation. It is tightly linked to language, reading, and academic skills. A landmark study by Catts et al. (2002) followed children with and without early language impairments and examined their reading and academic outcomes in adolescence. Although the study focused on broader language impairments rather than isolated articulation errors, it found that: children with early language delays were at substantially higher risk for reading disabilities and academic difficulties in later grades, and that early language status strongly predicted later outcomes.
While this research did not isolate speech sound disorders alone, it provides important context for understanding why speech sound milestones matter. Delays or persistent errors in speech sound development often co-occur with weaknesses in phonological processing, vocabulary, or sentence structure—skills that are foundational for reading. When speech sound milestones are significantly missed or progress stalls, they may serve as an early indicator of broader language vulnerabilities that can cascade into literacy challenges. For this reason, relying solely on a “wait-and-see” approach when milestones are not met may place a child’s long-term literacy trajectory at risk.
Articulation vs. Phonology: Two Sides of Speech Sound Development
Understanding the distinction between articulation and phonology helps explain why some children “can” say a sound in one word but not in another, or only in isolation.
Articulation
- Refers to the motoric, physical production of speech sounds.
- Involves coordinated movement of the tongue, lips, jaw, soft palate, and vocal folds.
- An articulation disorder usually involves consistent distortion or substitution of specific sounds due to motor pattern errors or structural constraints (for example, a lateral /s/, a dentalized /t/, or errors tied to cleft palate).
Phonology
- Refers to a child’s internal system of rules about how sounds function and combine in their language.
- A child may be physically capable of producing a sound but still omit, substitute, or simplify it in certain word positions or patterns due to immature phonological rules.
- A phonological disorder involves predictable patterns such as final consonant deletion or cluster reduction that persist beyond the expected age.
Clinically, articulation and phonology often overlap. However, the intervention approach differs: motor-based approaches target precise movements for specific sounds; phonological approaches target sound patterns and contrasts within the child’s system.
Key Speech Sound Milestones: When Should My Child Say Sounds?
Using normative data from ASHA, the Iowa–Nebraska norms, and Shriberg’s early–middle–late framework, we can outline approximate ages by which most children master specific consonants in English.
Early-Developing Sounds (Typically Mastered by 2–3 Years)
Most children correctly produce these sounds in words by age 2–3:
- p, b, m, n, h, w, d
Common early words containing these sounds include mama, no, bed, hat, book, bad.
These sounds require relatively simple, observable oral movement (for example, closing the lips for /p, b, m/) and often appear in the first 50 words of many children.
Middle-Developing Sounds (Typically Mastered by About 3–4½ Years)
Most children produce these correctly between approximately 3 and 4½ years:
- t, k, g, f, v, ŋ (“ng” as in “sing”), j (“y” as in “yes”)
Example words: cat, go, fun, give, sing, yes.
Normative data from Smit et al. (1990) and related sources show that velars (/k, g/), labiodentals (/f, v/), and the nasal /ŋ/ cluster in the middle range of acquisition, with growing consistency across word positions during the preschool years.
Later-Developing Sounds (Typically Mastered by About 5–7+ Years)
Most children master these later, with wider age ranges:
- s, z, ʃ (“sh”), tʃ (“ch”), ʒ (“zh” as in “measure”), dʒ (“j” as in “jump”), l, r, θ (“th” in “thin”), ð (“th” in “this”)
Example words: sun, zebra, shoe, cheese, measure, jump, love, red, think, this.
The “sibilants” and liquids (/s, z, ʃ, ʒ, tʃ, dʒ, l, r/) are more complex in terms of tongue shaping and airflow. “TH” sounds (/θ, ð/) often persist as substitutions (for example, /f/ for /θ/ in think) until the early school years. ASHA’s developmental guidance (“How Does Your Child Hear and Talk?”) summarizes that:
By age 8, children should correctly produce almost all sounds of English in everyday conversation.
Quick Speech Sound Milestones Chart
Sounds Mastered by Most Children By:
2–3 years: /p, b, m, n, h, w, d/
3–4.5 years: /k, g, f, t, v, ŋ, j/
5–6 years: /s, z, l/
6–7+ years: /r, ʃ, tʃ, dʒ, θ, ð/
To answer the main parent question “When should my child say sounds?”, we have put together a speech sound milestones chart that helps in guiding parents and clinicians in what to expect and when to help.
Typical Phonological Patterns vs. Red Flags
Children rarely move from babbling to perfect adult speech. Instead, they pass through a phase of phonological processes or simplification patterns. Many of these are typical and age-appropriate, provided they resolve “on schedule”.
Examples often cited in clinical practice include:
- Final consonant deletion
- Example: “ca” for “cat”
- Generally expected to resolve by about 3 years.
- Cluster reduction
- Example: “poon” for “spoon”
- Typically resolves by around 4 years
- Fronting
- Example: “tat” for “cat”
- Typically resolves by around 3 to 4 years.
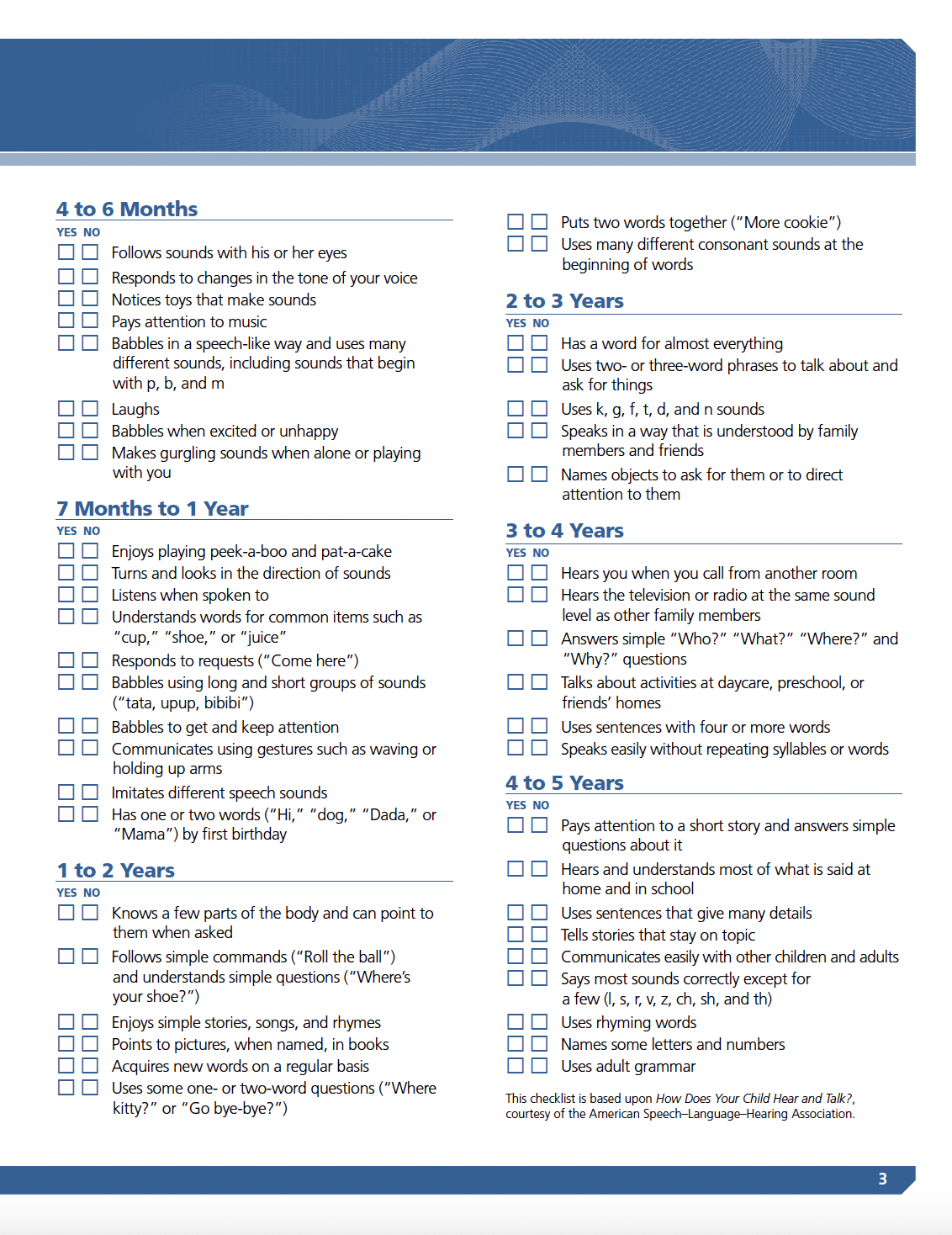
When these processes persist beyond expected ages, or when multiple processes markedly reduce intelligibility, a phonological disorder is suspected and parents might want to consider speech therapy. The National Institute on Deafness and Other Communication Disorders (NIDCD) provides a great checklist on your baby’s hearing and speech and language development, including typical variability and red flags
What Parents Notice Across Ages
Parents often seek support not because they can name a specific speech error, but because their child seems increasingly frustrated or difficult to understand. In many cases, the challenge isn’t identifying which sounds are wrong—it’s understanding why communication feels hard. What parents notice tends to shift with age, following predictable developmental patterns.
By age 2, children commonly use simplified word forms, such as saying “nana” for banana. While their sound inventory is still limited, there should be some variety in the consonants they use, and caregivers typically understand much of what the child is saying within familiar routines and contexts.
By age 3, speech often still sounds “immature,” but familiar listeners usually understand a large portion of what the child says. Processes such as final consonant deletion and cluster reduction may still occur, although they should begin to decrease over time.
By age 4, speech intelligibility improves significantly. Most unfamiliar listeners should understand the child during connected conversation. At this stage, persistent patterns such as fronting (e.g., “tat” for cat) or frequent cluster reduction across many words become more concerning.
By age 5, most early- and middle-developing sounds are expected to be in place. Errors on some later-developing sounds—particularly /r/ and “th” sounds—may still be within typical limits. However, consistent errors of /l/ or multiple mid-range sounds signal the need for closer evaluation. When this occurs, it’s important to consider not only which sounds are affected, but also the underlying factors that may be influencing a child’s speech development.
Factors Influencing Speech Sound Development
Speech sound milestones vary across children, and development is shaped by more than age alone. One of the most well-documented influences on articulation and phonology is hearing status, as accurate speech production depends on consistent access to clear auditory input.
Even mild or fluctuating hearing loss can interfere with how children perceive and learn speech sounds. Research on pediatric hearing loss highlights several key points:
- Conductive or sensorineural hearing loss can cause children to misperceive speech sounds, which directly affects how those sounds are produced.
- Inconsistent or reduced auditory input may lead to persistent articulation errors or broader phonological pattern delays.
- Children with undetected or unmanaged hearing loss are at increased risk for ongoing speech sound difficulties, particularly if intervention is delayed.
Because hearing loss in young children may be subtle or temporary (for example, related to recurrent ear infections), its impact on speech development can be overlooked. Early identification and management play a critical role in supporting typical speech sound acquisition.
Orofacial Structure and Function
In some children, speech sound errors are not solely developmental but are influenced by structural differences of the oral–facial mechanism. When the anatomy involved in speech production is altered, certain sounds may be more difficult—or impossible—to produce accurately without targeted support.
Structural differences that can affect speech sound development include:
- Cleft lip and/or palate, which can disrupt airflow and pressure needed for production of certain consonants
- Significant malocclusion, which may alter tongue placement and jaw stability for precise articulation
- Tongue-tie (ankyloglossia), which can restrict tongue movement required for certain speech sounds
These structural differences are often associated with sound-specific articulation difficulties, particularly for pressure consonants that rely on controlled airflow and oral closure. Because the underlying issue is anatomical rather than developmental, speech errors may persist despite typical maturation.
Targeted intervention and multi-disciplinary approach involving speech-language pathologists and medical specialists are essential when structural anomalies are suspected. Early identification allows for appropriate referral, coordinated care, and individualized intervention planning to support optimal speech outcomes.
Linguistic and Environmental Input
Speech sound development is closely tied to the child’s language environment. Rich, interactive communication—where adults respond, expand, and engage meaningfully with a child’s attempts—supports both sound learning and broader language growth. While the exact “dose” of language exposure needed for optimal speech development can not be quantified, a consistent finding across developmental research is that responsive, language-rich environments foster stronger communication skills over time. Longitudinal work on language and literacy development, including studies examining later reading outcomes, reinforces the importance of early oral language experiences as a foundation for academic success.
Co-Occurring Developmental Conditions
Some children experience speech sound difficulties as part of a broader developmental profile rather than in isolation. Children with the following conditions are at higher risk for more complex or persistent speech sound disorders:
- Global developmental delay
- Autism spectrum disorder (ASD)
- Childhood apraxia of speech (CAS)
In these cases, speech sound errors may reflect underlying differences in motor planning, neuromuscular control, sensory processing, or language development. Because speech patterns can look similar on the surface but stem from different causes, comprehensive assessment by a speech-language pathologist is essential to differentiate between conditions and guide appropriate intervention. While precise prevalence rates vary and are beyond the scope of the cited sources, the increased risk associated with these conditions is well recognized in clinical practice.
When to Worry: Evidence-Informed Red Flags
While speech development varies from child to child, research and clinical guidance from ASHA, NIDCD, and the broader speech-language literature consistently point to several red flags that warrant closer attention. These signs suggest that speech sound difficulties may be more than a temporary developmental difference.
Key red flags include:
- A very limited consonant inventory by age 2, such as using only a few consonant sounds or relying heavily on vowels.
- Speech that remains largely unintelligible to caregivers by age 3, even when the listener knows the child well and understands the context.
- Speech that is difficult for unfamiliar listeners to understand by age 4, particularly during connected conversation.
- Persistent speech sound errors beyond expected milestones, such as little to no progress with mid-range sounds after age 5 or minimal improvement across an entire school year.
- Observable frustration, withdrawal, or reluctance to speak, which may signal that ongoing communication breakdowns are affecting the child’s social or emotional well-being.
The importance of recognizing these warning signs is reinforced by population-based research. A large study by McLeod and Harrison (2009) documented the prevalence and associated risk factors of speech sound disorders in children, underscoring that these difficulties are common and carry meaningful developmental impact when left unaddressed. While the study focuses on prevalence rather than intervention outcomes, its findings highlight the public health significance of early identification and timely support.
When one or more of these red flags are present, referral to a speech-language pathologist should not be delayed. Early evaluation helps clarify whether errors fall within expected developmental variation or reflect a speech sound disorder that would benefit from intervention.
Research-Supported Strategies to Support Speech Sound Development
Although high-quality randomized trials do not exist for every possible home strategy, several practice recommendations are consistently supported by broader speech, language, and literacy research. These approaches emphasize responsive interaction, consistent modeling, and developmentally appropriate support rather than correction or trying to fix it.
Model, Do Not Pressure: Recasting
Recasting involves repeating what a child says with a correct or more complete form, without demanding imitation.
- Child: “Tat!”
- Adult: “Yes, cat. I see the cat.”
ASHA’s parent resources emphasize modeling and expansion rather than repeated “say it again” demands, particularly for toddlers and preschoolers, reflecting research showing that adult language modeling and expansion of children’s utterances fosters communication more effectively than pressure to imitate.
Why it matters:
Recasting keeps communication natural and low-pressure while repeatedly highlighting accurate adult forms. This aligns with broader language intervention principles: high-quality input, frequent models, and responsive interaction.
Expand and Elaborate
Expansion builds on what a child says by adding words, grammar, and detail—supporting both speech sound development and language structure.
- Child: “Dog run.”
Adult: “Yes, the dog is running fast. The big brown dog is running.”
Expansion and extension are accessible, everyday strategies that increase children’s exposure to correct grammar, vocabulary, and speech sounds within real communication.
Visual and Tactile Cues for Articulation
Many motor-based speech intervention approaches incorporate visual and tactile cues to provide tangible feedback:
- Using a mirror so children can see lip and tongue placement
- Drawing simple mouth diagrams for specific sounds
- Using tactile cues (e.g., touching the throat to highlight voicing for /z/ vs. /s/)
Cues such as “look at my mouth” and simple explanations on how to say a sound can help children understand how sounds are made.
Build a Language-Rich, Low-Noise Environment
Daily routines can support speech and language learning in a naturalistic way:
- Shared book reading with exaggeration of target speech sounds
- Singing songs, using rhymes, and playing sound-based games
- Reducing background noise (TV, loud music) so children can hear speech clearly
While individual strategies are not always isolated in experimental studies, the broader language and literacy literature consistently links rich oral language exposure in early childhood to later reading and academic success.
Playful Sound-Focused Activities
Play based activities are great ways to increase awareness and speech sound development during parent-child interactions.
- “I Spy”: “I spy something that starts with /r/ sound.”
- Sound sorting: Grouping pictures or objects by beginning sounds
- Prosodic play: Whispering, shouting, or changing pitch on target words
These activities strengthen phonological awareness while keeping practice engaging, repetitive, and child-centered.
Evidence-Based Intervention Approaches for SLPs
When children miss key speech sound milestones, speech-language pathologists rely on structured, research-informed intervention approaches rather than trial-and-error techniques. A comprehensive narrative review by Wren, Roulstone, and Gibbon (2019) examined the existing evidence base for interventions targeting childhood speech sound disorders, offering important insight into what works—and why.
The evidence supported several well-established intervention approaches, including:
- Phonological contrast therapies, such as minimal pairs
- The Cycles Phonological Approach
- Motor-based articulation therapy using structured, repetitive practice
The conclusion supported the notion that targeted, theory-driven interventions lead to measurable improvements in children’s speech accuracy when applied systematically and monitored carefully.
Current clinical practice approaches such as minimal pairs, cycles, and motor-based treatments remain appropriate and effective tools when selected based on a child’s specific speech profile and implemented with intention and consistency.
Common Evidence-Supported Components Across Approaches
Across the intervention literature summarized several core elements of effective speech sound intervention consistently emerge. Regardless of the specific approach used, successful therapy tends to share these foundational features:
- Focused practice on specific targets
Intervention begins with identifying priority speech sounds or phonological patterns based on developmental norms and the child’s functional communication needs. - High repetition and treatment intensity
Children are given multiple, meaningful opportunities within each session to produce target sounds accurately, supporting motor learning and phonological change. - A structured cueing hierarchy
Therapy typically progresses from auditory discrimination and awareness to production at the syllable, word, phrase, and conversational levels, with cues systematically reduced as accuracy improves. - Emphasis on generalization and home practice
Effective intervention extends beyond structured drill. Targets are practiced in natural communication contexts, and caregivers are involved in brief, consistent home activities to help consolidate and maintain gains.
Together, these elements help explain why different evidence-supported approaches—such as phonological and motor-based interventions—can be effective when implemented systematically and monitored over time.
Home Practice and Family Involvement
Does intensity and practice matter? Evidence indicates that speech sound intervention is more effective when practice is frequent, targeted, and sufficiently intensive. A randomized controlled study by Allen (2013) found that preschool children with speech sound disorders made significantly greater phonological gains when therapy was delivered multiple times per week, even when total treatment time was held constant.
Broader evidence reviews reinforce this pattern. A systematic review by Kaipa and Peterson (2016) concluded that higher treatment intensity is generally associated with more favorable outcomes for children with speech sound disorders and childhood apraxia of speech, although “optimal” dosage parameters remain an area for continued research.
Across these studies and evidence syntheses, several common features of effective intervention emerge:
- High practice dose within sessions. Many successful interventions provide dozens of opportunities per session for children to produce target sounds accurately, supporting learning through repetition.
- Increased session frequency. Interventions delivered multiple times per week tend to yield stronger gains than less frequent schedules, particularly for phonological targets.
- Carefully structured practice conditions. Therapy is most effective when targets are clearly defined, practice is intentional, and difficulty is adjusted as accuracy improves.
While the research does not prescribe a single formula for home practice, it supports the broader clinical principle that consistent, well-planned practice—both in therapy and supported at home—helps children make and maintain progress. Collaboration between speech-language pathologists and caregivers is therefore an important component of effective intervention, ensuring that practice outside of sessions reinforces—not replaces—professional treatment.
In-Person vs. Online (Telepractice) for Speech Sound Disorders
While the studies cited above largely predate widespread telepractice, ASHA’s professional guidance acknowledges telepractice as an appropriate service delivery model for speech-language pathology when it meets professional, ethical, and technical standards.
When speech therapy is delivered via telepractice, speech language pathologists need to ensure that in-person and online sessions use the same underlying interventions (for example, minimal pairs, motor-based drill, cycles). The difference lies in delivery mode, not the core techniques. While parents need to ensure that the home environment and computer has:
- high speech internet and high-quality audio so subtle sound differences are audible.
- quiet environment and visual access to the child’s face for articulation cues.
- access to materials needed during the sessions (e.g., worksheet printouts)
Properly implemented, tele-practice can yield comparable outcomes for many children with mild or moderate speech sound disorders. However, severe speech sound disorders or complex motor speech issues may still benefit from in-person assessment and in-person treatment
In Summary: What Do Speech Milestones Tell Us
Speech sound milestones are not arbitrary age cutoffs or isolated skills to “check off.” They reflect how a child’s speech sound system is organizing and supporting communication—and they are closely connected to later language, literacy, and academic outcomes. Research consistently shows that early speech and language skills form a foundation for reading and learning, making early identification and support critically important when development falls outside expected ranges.
Understanding articulation and phonology helps explain why children may show varied progress: producing some sounds accurately while omitting or substituting others, or using correct sounds in one context but not another. Normative frameworks allow clinicians to interpret these patterns developmentally rather than relying on guesswork or comparison to peers.
Speech development also does not occur in isolation. Hearing status, oral–facial structure, language input, and co-occurring developmental conditions all shape how speech sounds are learned and used. The evidence reviewed throughout this guide points to a consistent conclusion: when speech sound difficulties fall outside expected developmental patterns, targeted, evidence-based intervention improves outcomes. Waiting without monitoring may increase the risk that challenges compound rather than resolve.
Final Takeaway: Speech Sound Parents Tips
Parents should not try to diagnose speech sound disorders—but they can use developmental milestones to make informed decisions and seek help if needed.
- Use speech sound patterns, not just age, as your reference point. Pay attention to which sounds your child uses consistently, which are missing, and whether speech is becoming clearer over time. Persistent omissions, substitutions, or reduced intelligibility beyond expected ages are worth discussing with a speech-language pathologist.
- Prioritize consistent modeling in everyday interactions. Responding to your child’s speech with accurate, expanded models—without pressure to repeat—supports learning while keeping communication positive and natural. Consistency across daily routines matters more than correction.
- Create listening-friendly environments. Reducing background noise, engaging in shared book reading, and setting aside small daily windows for focused interaction help children hear and process speech more clearly.
- Take home practice seriously when it is recommended. Research shows that structured, targeted practice supports progress, especially when it is specific, and consistent. When a speech therapist assigns a home routine, it is designed to reinforce—not replace—therapy.
- Monitor intelligibility outside the family circle. How well unfamiliar listeners understand your child provides important information. Frequent breakdowns with teachers, peers, or extended family members should be shared with your speech-language pathologist to guide next steps.
When speech sound errors persist beyond expected milestones, significantly reduce intelligibility, or cause frustration or withdrawal, early evaluation and targeted support are crucial in supporting your child’s communication.
Speech sound milestones are best used as a tool for understanding and informed decision making. With the right framework, timely monitoring, and collaboration between families and professionals, children can be supported in developing effective communication that spans across lifetime.



.svg)
.svg)
